The BRIC countries, namely Brazil, Russia, India and China, have received a lot of attention since the acronym was coined by Jim O’Neil in 2001; he was, at the time, the Head of Global Economic Research at Goldman Sachs and he used it to refer to what he predicted would be the fastest growing emerging economies in the world. In 2006, the four countries met for the first time and adopted the acronym ‘BRIC’ in a bid to formalize their union and increase their stature. They held their first official summit in Russia in June 2009, debuting as a policy consultation and coordination group; and since then have shown interest in building a platform for cooperation on issues such as health, economics, science and technology. In 2010, South Africa was formally invited to join the BRIC countries by the president of China making the BRIC, the BRICS.
Since their emergence as a group, many commentators have championed the BRICS as good news for global health. However, this article seeks to explore whether it is right to assume that their economic accolades readily extend to the sphere of Global Health.
Over the last decade, while there have been a variety of groups of emerging countries making a mark on the global economic landscape, the BRICS seem to have made the most notable impact. Their economies grew at an average of 6% annually between 2000 and 2010, much faster than the growth of the Organisation for Economic Co-operation and Development (OECD) economies, which grew by an average of 2% annually during the same time period. Combined, the BRICS account for 19% of nominal world Gross Domestic Product (GDP), with China, Brazil and India ranking among the top 10 economies in the world by nominal GDP. While there are signs of these phenomenal economic growth rates slowing, the BRICS continue to grow in political stature.
As well as their overall economic development, the BRICS have increased their international development cooperation. In 2010 alone, they spent over US$6 billion on foreign assistance to low- and middle-income countries (directed primarily towards health, education, infrastructure, information technology, agriculture, training and capacity building) and this foreign assistance grew steadily by an average of 16% annually (excluding Russia) between 2005 and 2010.1
Individual BRICS countries are becoming more vocal and active in shaping, and indeed leading, global (read ‘worldwide’) health movements
Although the foreign assistance spending of the BRICS is relatively small when compared to the foreign aid spending of other major donors such as the United States (US$30.7 billion in 2011) or OECD’s thirty-four member countries (US$133.5 billion collectively in 2011), it is still substantial and worthy of note. Moreover, with aid donations from the OECD countries to developing countries, known as Official Development Assistance, declining for the first time in 15 years and health spending cuts being made by most European governments due to financial constraints, the world seems to be looking to the BRICS as the next set of potential donors and health innovators.
During the first BRICS Health Ministers’ meeting held in Beijing in 2011, the BRICS made a statement reiterating their firm commitment to strengthen dialogue and cooperation in the field of public health. At the summit Dr Margret Chan, the Director-General of the World Health Organization said “… BRICS represents a block of countries with a … great potential to move global public health in the right direction … towards reducing the current vast gaps in health outcomes and introducing greater fairness in the way the benefits of medical and scientific progress are distributed …”.2
It is important to note that while the BRICS may be building their profile as health donors, they continue to face significant domestic health challenges of their own. Two of the most prominent issues include the dominance of non-communicable diseases compared to the burden of infectious diseases (apart from in South Africa) and their ageing populations.
Are the BRICS a Collective Force in Global Health?
The question then arises whether the BRICS, lauded for their economic achievements, qualify as global health champions?
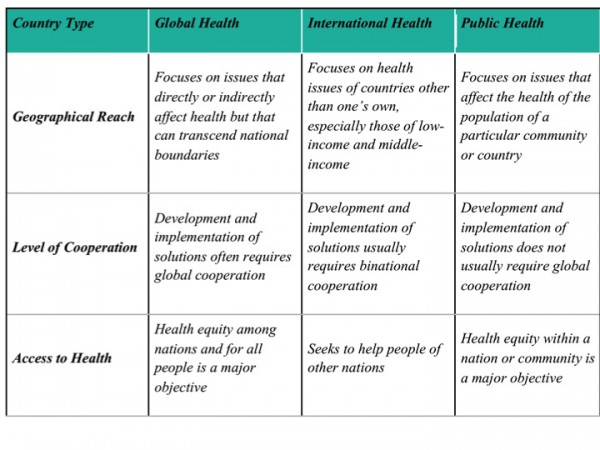
To answer this question, what is meant by the term global health needs to be clarified. This requires understanding how the word ‘global’ differs from words that are commonly conflated with ‘global’ such as ‘international’ and ‘public’. Our analysis of the BRICS reveals that the label ‘global health’ continues to be attached indiscriminately to what are really either public/national or international health issues. The reader is provided with two useful analyses that should set them on the right track. The first is a framework that distinguishes between global, international and public health (see box above).3 The second is a highly nuanced analysis of the different ways that the word ‘global’ is used to describe global health,4 which is itself subject to a favourable critique by Rowson et al (2012) (see table below).5
So, are the BRICS a collective force in global health? Well, as argued above, it depends on what is meant by global. Examples from the literature that describe the BRICS countries’ influence as global include Brazil’s leading role in the negotiations that led to the Framework Convention on Tobacco Control; India, Brazil and South Africa’s involvement in issues around access to anti-retroviral drugs, resistance to the dominant intellectual property rights regime and support for generic drug manufacture; India’s support for low cost service delivery and ‘frugal innovation’ such as that pioneered by the Aravind eye hospital; and China’s international medical teams. But to what extent are these ‘global’ interventions or actions?
Drawing on Bozorgmehr’s four definitions of ‘global’, it seems to us that most of the examples of the BRICS so-called ‘global’ influence in health are actually international actions incorrectly relabelled as global; or are issues that simply cross national borders (typically infectious diseases); are issues that are global but in the limited sense that they are ‘worldwide’; or are described as global when really they are public health interventions, plain and simple. Very few commentaries on BRICS have identified the significance of their actions in terms of supra-territoriality.
Little evidence is found in literature to support the assertion that the BRICS are influencing global health as a ‘block’
A full answer to the question would also have to consider the extent to which the BRICS coordinate their efforts towards improving global health. True, each of the BRICS countries engages individually in bilateral, trilateral and multilateral efforts to improve health, although some members prefer one channel of assistance to another: Russia channels its development assistance almost exclusively through multilateral partnerships such as the Global Fund to Fight AIDS, Tuberculosis and Malaria, while China is less active in its multilateral or trilateral engagement, preferring traditional bi-lateral relations. Furthermore, individual BRICS countries are becoming more vocal and active in shaping, and indeed leading, global (read ‘worldwide’) health movements such as Universal Health Coverage or the support for generic drug production.
But what about the BRICS’collective action for global health? Little evidence is found in literature to support the assertion that the BRICS are influencing global health as a ‘block’.6 7 Joint statements by all five of the BRICS are rare: there have been just two Health Ministers high-level meetings. More common are examples of two or more BRICS countries supporting specific health initiatives, and here the preferred channel of influence is multilateralism. The Global Polio Eradication Initiative (GPEI) is one example of a multilateral initiative and a global partnership for health that is supported by two BRICS countries: India and Russia. And in the context of reform of the World Health Organisation, BRICS Ministers of Health committed “to strengthen and legitimize the WHO as the coordinating authority in global health” through the principle of multilateralism.8
All of this is not to say that the various Summits and High Level Meetings of BRICS Political leaders or Communiqués issued by Ministers of Health are without meaning or import for global health. Such international fora – and we would emphasise that they are international agreements between states – do show political will for collective action. But it is one thing to commit to do something; quite another to actually put those commitments into action. Here we agree with a conclusion drawn by the authors of a recent Report on BRICS and Global Health: “The BRICS have declared health collaboration a priority, but they have not yet begun to work collectively to enhance the impact of their assistance programs”.1

In 1955 in Bandung, Indonesia, developing countries met for the first time to promote economic and cultural cooperation and to oppose colonial resurgence from either the US or the Soviet Union as the Cold War played out. TheBandung Conference, as it became known, is also credited as sowing the seeds for the Non-Aligned Movement (a movement that sought to radically shift the Western discourse of ‘development’). For many BRICS-watchers, the groups’ most significant contribution has been to re-frame development through a counter discourse that rejects Western notions of ‘aid’, promotes horizontal rather than vertical assistance, partnership, non-conditionality, and heavily promotes values such as equity. If the BRICS have collective influence in global health, then it is most likely to be found in this realm of ideas and discourse; extending into the health sphere a counter-discourse of health cooperation. But, as Mawdsley (2012)9 argues, the coherence amongst BRICS of a common discourse of health development should not be exaggerated.
Conclusion
Although there is limited evidence of the BRICS working as a team of five countries, there are examples of initiatives in which certain members do work together. The BRICS as individual countries have a history of contributing to health improvements of countries beyond their borders long before labels such as ‘Global Health’ and ‘BRICS’ were popularised. Their actions both directly and indirectly have affected the health of populations in other low and middle income countries in areas such as infrastructure building, capacity building and health innovation. However, we find a tendency in much of the literature on BRICS and ‘global health’ to describe interventions by one or more of the BRICS countries as global when a more accurate term such as international would be appropriate.
While it might be a little premature to look to the BRICS collective as current global health champions, they appear to have ambitions of moving in this direction. How far their influence will extend into the supraterritorial sphere – i.e. enabling people to become physically, legally, culturally, and psychologically engaged with each other in ‘one world’10 – remains to be seen.